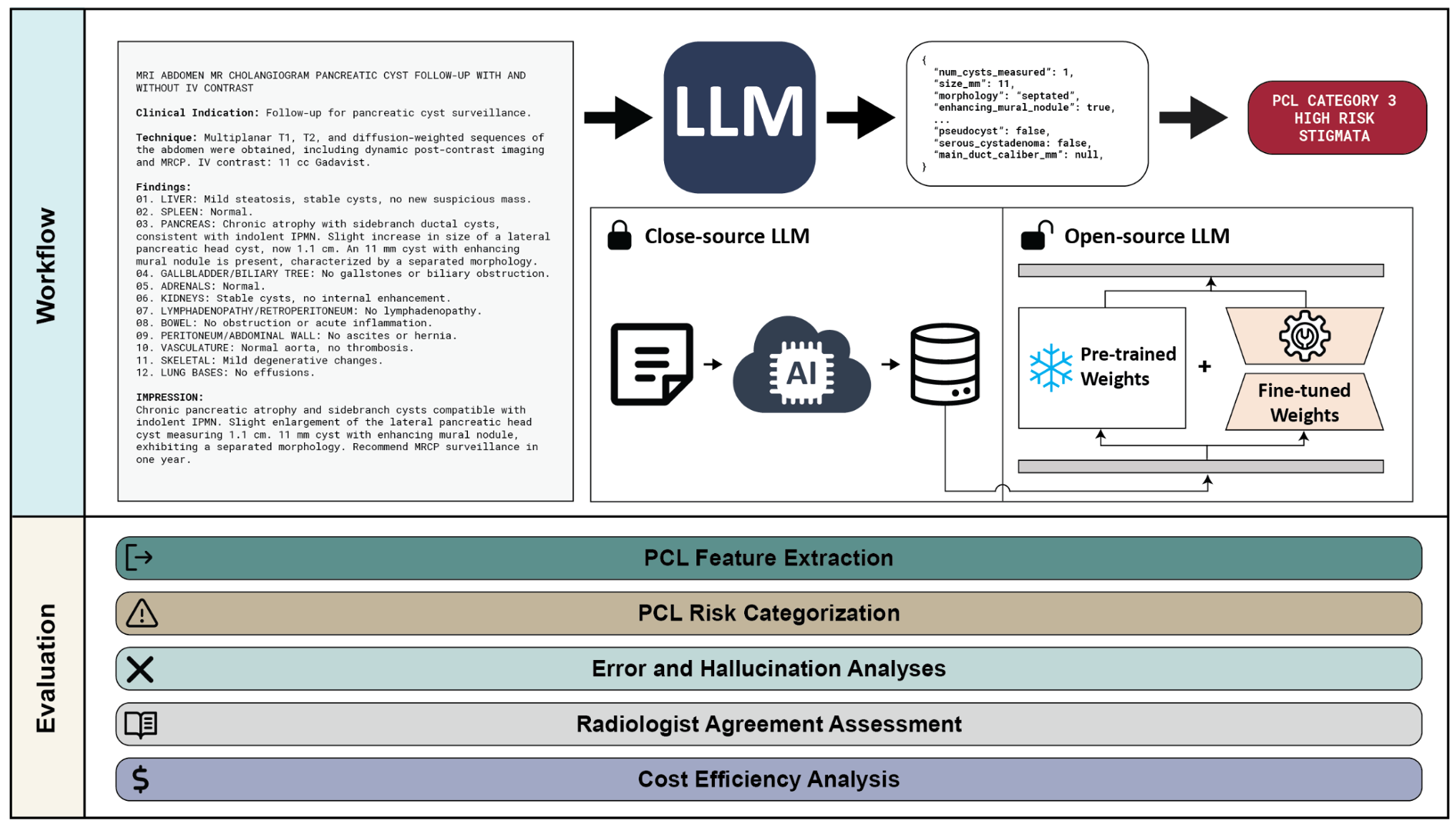
Figure 1. We developed and evaluated an LLM-based system for the automatic extraction and risk categorization of pancreatic cystic lesions (PCLs) from radiology reports. The system processes free-text reports to extract clinically relevant PCL features, which are then mapped to risk categories based on established guidelines. We evaluated both proprietary (GPT-4o) and open-source (LLaMA, DeepSeek) models, including fine-tuned variants, across five dimensions: PCL feature extraction accuracy, PCL risk categorization performance, error and hallucination analyses, radiologist agreement assessment, and cost-efficiency. Fine-tuned models achieved feature extraction accuracy comparable to GPT-4o (LLAMA-FT: 97% [95% CI: 97–98%], LLAMA-FT-CoT: 97% [97–98%], DeepSeek-FT-CoT: 98% [97–98%], GPT-CoT: 97% [97–98%]). Risk categorization F1 scores were similarly high (LLAMA-FT: 0.95 [0.91–0.98], LLAMA-FT-CoT: 0.93 [0.89–0.97], DeepSeek-FT-CoT: 0.94 [0.90–0.98], GPT-CoT: 0.97 [0.93–0.99]). The radiologist agreement assessment showed strong agreement between models and expert radiologists (Fleiss’ kappa: radiologists alone = 0.888; radiologists + DeepSeek-FT-CoT = 0.893; radiologists + GPT-CoT = 0.897), indicating LLM-derived outputs are on par with expert interpretation.
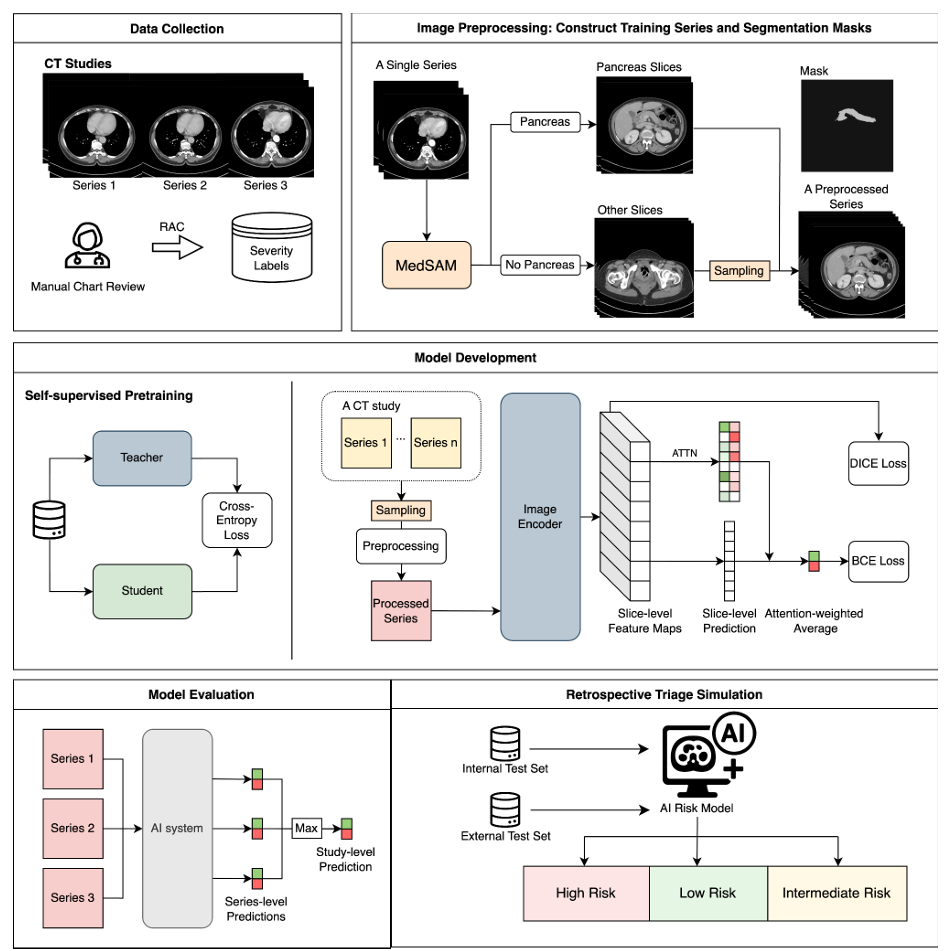
Figure 2. Workflow of the AI system. Data Collection: CT studies with multiple series were used in this study. Severity labels were assigned based on the Revised Atlanta Classification (RAC). Image Preprocessing: During training, MedSAM, an automated deep learning segmentation model, was used to generate pancreas masks and identify relevant slices. These were combined with randomly sampled non-pancreas slices to create preprocessed input series. Segmentation is not required at inference time. Model Development: A transformer-based backbone (pretrained via self-supervised learning) extracted slice-level features. Slice scores derived from saliency maps were aggregated using attention (ATTN) to generate severity predictions, optimized with binary cross entropy (BCE), Dice, and L1 losses. Model Evaluation: Study-level predictions were generated by using the maximum series-level score. Retrospective Triage Simulation was performed on both internal and external test sets.

Project Lead
